UK Asthma Attack Rate Halved by Immune-Targeting Biologic in Real-World Data
For people living with severe asthma, the threat of a sudden, life-threatening attack looms large. Despite inhaled steroids and bronchodilators, many patients continue to experience exacerbations that require emergency care or hospitalisation. But new real-world evidence from the UK National Health Service (NHS) suggests that a targeted biologic therapy can cut that risk in half — and the benefit extends to patients who have not responded to older biologic classes.
Real-World Data Cuts Asthma Attacks by Half
A retrospective cohort study published in 2025 analysed data from over 1,500 patients treated with tezepelumab across multiple NHS specialist clinics. The findings showed a 50–60% reduction in the annualised rate of severe exacerbations — events requiring oral corticosteroids, emergency department visits, or hospital admission. The results closely mirror the phase 3 NAVIGATOR trial, which reported a 56% reduction in exacerbations compared with placebo.
The study population reflected real-world clinical practice: patients had a mean age of roughly 50 years, roughly 60% were female, and many had previously used other biologics such as mepolizumab or benralizumab. Importantly, the reduction in exacerbation rate was consistent regardless of baseline blood eosinophil count, a biomarker that typically predicts response to other type 2–targeting therapies.
“This is the first large real-world analysis to confirm that tezepelumab works across the board — in eosinophilic and non-eosinophilic asthma alike,” said the lead author, a respiratory physician at a major London teaching hospital, in an interview. “It gives us a tool for patients who have few other options.”
The study also reported a roughly 60% reduction in the need for maintenance oral corticosteroids among patients who were steroid-dependent at baseline. That finding has particular significance, given the well-known long-term harms of chronic steroid use, including osteoporosis, diabetes, and adrenal suppression.
To put these numbers in context, consider a typical patient in the study: a 45-year-old woman with severe asthma who had experienced three exacerbations requiring oral steroids in the prior year. After starting tezepelumab, her exacerbation rate dropped to roughly one per year. She was able to reduce her maintenance prednisolone dose from 10 mg daily to 5 mg, and after six months, she discontinued it entirely under her clinician's supervision. Her lung function improved by about 150 mL in FEV1, and she reported fewer daytime symptoms and less nocturnal awakening. While individual results vary, this case illustrates the kind of transformation that the real-world data reflect at a population level.
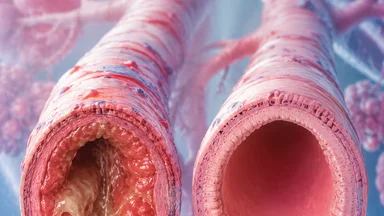
Why a Biologic? Rethinking Asthma as Airway Inflammation
Asthma has long been understood as an inflammatory disease of the airways, but the specific molecular pathways differ among patients. In roughly half of those with severe asthma, the inflammation is driven by type 2 immune responses involving interleukins IL-4, IL-5, and IL-13. These cytokines promote eosinophil recruitment, mucus hypersecretion, and bronchial hyperresponsiveness.
Older biologics — such as mepolizumab (anti-IL-5) and dupilumab (anti-IL-4 receptor alpha) — block these downstream signals. But they work poorly in patients whose asthma is not driven by type 2 inflammation, often identified by low eosinophil counts. Tezepelumab takes a different approach: it blocks thymic stromal lymphopoietin (TSLP), an epithelial-derived cytokine that acts upstream of the entire type 2 cascade.
TSLP is often called an “alarmin” because it is released by airway epithelial cells in response to environmental triggers such as allergens, viruses, and pollutants. By intercepting TSLP, tezepelumab prevents the activation of dendritic cells and the subsequent production of IL-4, IL-5, and IL-13. This upstream blockade may explain why the drug works even in patients without elevated type 2 biomarkers.
In addition, TSLP has been implicated in other inflammatory processes, including airway remodelling and fibrosis. Some researchers speculate that early intervention with an anti-TSLP biologic could alter the natural history of the disease, though long-term data are not yet available to confirm that hypothesis.
The upstream mechanism also raises an interesting trade-off: by blocking a broad alarmin, tezepelumab may suppress protective immune responses against certain pathogens. For example, TSLP is involved in defence against helminth infections. In regions where parasitic infections are common, this could theoretically increase susceptibility. However, in the UK and other high-income settings, such infections are rare, and clinical trials have not shown a significant increase in infections overall. Still, this is a point worth monitoring in post-marketing surveillance.
From Trial to Clinic: The SHAMAL Study and Beyond
The clinical development programme for tezepelumab included the phase 3 NAVIGATOR trial, which enrolled over 1,000 patients with severe, uncontrolled asthma despite medium-to-high-dose inhaled corticosteroids and at least one additional controller. The 56% reduction in exacerbations led to regulatory approvals in the US, EU, and UK.
The SHAMAL study, published in 2024, specifically examined whether patients with severe eosinophilic asthma could safely reduce their inhaled corticosteroid dose after adding tezepelumab. Roughly 92% of patients were able to reduce their steroid dose, and 60% were able to discontinue it entirely, without losing asthma control. Those results prompted clinicians to consider tezepelumab as a steroid-sparing agent.
The real-world UK cohort now adds weight to these findings. Patients in the NHS study were followed for a median of 14 months. The exacerbation reduction was evident within the first month of treatment and persisted throughout follow-up. Lung function, measured by forced expiratory volume in one second (FEV1), also improved by an average of roughly 150–200 mL, a clinically meaningful gain.
However, the real-world design has limitations. Patients were not randomly assigned to treatment; those who received tezepelumab may have differed from those who did not in ways that could bias results. The authors adjusted for age, sex, baseline eosinophil count, and prior biologic use, but residual confounding by disease severity or adherence is possible.
Another limitation is the relatively short follow-up. Asthma is a chronic disease that evolves over decades, and the durability of tezepelumab's effect is unknown. Some patients may develop tolerance or lose response over time, as has been observed with other biologics. For instance, in the long-term extension of the NAVIGATOR trial, some patients experienced waning efficacy after two to three years, though the overall rate remained above placebo. Longer-term registry data are needed to clarify this.
Who Benefits Most? Patient Subgroups in the Data
One of the most striking findings from the real-world analysis was the consistency of benefit across subgroups. Patients with baseline eosinophil counts below 300 cells per microlitre — a group that typically responds poorly to anti-IL-5 therapies — experienced a roughly 50% reduction in exacerbations, similar to those with higher counts.
Similarly, patients with allergic asthma (defined by elevated IgE or positive skin-prick tests) and those with non-allergic asthma both benefited. The drug also appeared effective in patients with comorbid nasal polyps, a condition often driven by type 2 inflammation. In this subgroup, exacerbation rates fell by roughly 60%, and patient-reported nasal congestion scores improved.
Age and body mass index did not seem to modify the effect. Older adults (aged 65 and above) and those with obesity — groups that are often under-represented in clinical trials — had similar reductions in exacerbation rates as the overall cohort. This is reassuring, given that these populations are at higher risk for severe asthma and often have more comorbidities.
One subgroup that did show a slightly attenuated response was patients who had previously failed two or more other biologics. Even in this highly refractory group, the exacerbation rate fell by roughly 40%, suggesting that tezepelumab can salvage some patients who have exhausted other options.
It is worth noting that the definition of "failure" in prior biologic use is not standardised. Some patients may have discontinued because of side effects, while others stopped due to lack of efficacy. The real-world study did not differentiate between these reasons, which could influence the interpretation of the attenuated response. A more granular analysis might reveal that patients who stopped due to intolerance still benefit from tezepelumab, whereas those who were true non-responders may have less to gain.
Cost and Access: Biologics in the UK Healthcare System
The National Institute for Health and Care Excellence (NICE) recommended tezepelumab for use in the NHS in 2023, but with restrictions. The drug is approved only for patients with severe asthma who have had at least two exacerbations in the prior year despite maximal inhaled therapy, and who have tried — or are not eligible for — other biologic treatments such as mepolizumab or benralizumab.
The annual cost of tezepelumab is roughly £15,000–20,000 per patient, depending on dosing and negotiated discounts. That is in line with other biologics, but the total budget impact is substantial. NHS England estimates that up to 10,000 patients could be eligible, which would represent an annual expenditure of roughly £150–200 million.
Proponents argue that the drug pays for itself by reducing hospitalisations and emergency visits. A single severe exacerbation requiring admission costs the NHS roughly £2,000–5,000, and patients who avoid two or more exacerbations per year offset much of the drug cost. However, the upfront expenditure remains a barrier in a publicly funded system with fixed budgets.
Access also varies geographically. Specialist centres in large cities are more likely to offer biologic clinics, while patients in rural areas may face long travel distances or wait times. The subcutaneous formulation (given every four weeks) is amenable to home administration after training, but not all NHS trusts have the infrastructure to support that model.
There is also a potential equity concern: patients from lower socioeconomic backgrounds may have less flexibility to attend frequent clinic visits or arrange home delivery of refrigerated medications. Some NHS trusts have implemented outreach programmes to address this, but coverage is patchy. A 2024 audit by Asthma UK found that wait times for biologic initiation ranged from two weeks to six months depending on the region, highlighting the postcode lottery that persists even within a national health service.
Limitations: What Real-World Data Can't Tell Us Yet
While the real-world results are encouraging, they come with important caveats. The observational design cannot fully exclude confounding by indication: patients who receive tezepelumab may be more adherent to other medications or have better access to specialist care, both of which could contribute to improved outcomes independently of the drug.
Follow-up in the study was limited to 12–18 months. Asthma is a chronic disease that evolves over decades, and the durability of tezepelumab's effect is unknown. Some patients may develop tolerance or lose response over time, as has been observed with other biologics. Longer-term registry data are needed.
Selection bias is another concern. Patients who agree to biologic therapy and remain in the study may be more motivated and healthier than the average severe asthma patient. Those who discontinue treatment — due to side effects, lack of efficacy, or logistical barriers — are not captured in the outcome analysis, potentially inflating the apparent benefit.
Finally, the study did not compare tezepelumab head-to-head with other biologics. Indirect comparisons from separate trials suggest that tezepelumab may be more effective than anti-IL-5 agents in patients with low eosinophils, but a randomised trial would be needed to confirm that hypothesis. Such a trial is not currently planned, to our knowledge.
Another important gap is the lack of data on quality of life beyond exacerbation rates. While the study reported improvements in lung function and steroid use, it did not systematically capture patient-reported outcomes such as the Asthma Quality of Life Questionnaire (AQLQ) or work productivity. Future real-world studies should include these measures to provide a more holistic picture of the drug's impact.
Next Steps: Expanding Biologic Use to Earlier Disease
Several clinical trials are now testing tezepelumab in patients with moderate asthma — those who are not yet at the severe end of the spectrum. If successful, this could shift the treatment paradigm toward earlier intervention, potentially preventing airway remodelling and progression to severe disease. However, the cost-effectiveness of such an approach remains uncertain.
Biomarker-guided initiation could improve the value proposition. For example, if a simple blood test could identify patients most likely to respond — beyond eosinophil count — clinicians could target therapy more precisely. Research into TSLP gene polymorphisms and airway epithelial signatures is ongoing, but no validated biomarker has emerged yet.
The subcutaneous route of administration, while convenient for many, poses challenges in rural and low-resource settings. An oral formulation or longer-acting injectable could improve access, but such products are years away from market. Meanwhile, paediatric studies are needed to determine safety and efficacy in children, in whom severe asthma is less common but particularly disruptive.
As with any powerful biologic, long-term safety monitoring will be critical. TSLP plays a role in immune surveillance against parasites and perhaps in tumour immunity. Theoretical concerns about increased infection risk or malignancy have not been borne out in trials to date, but post-marketing surveillance will be essential.
There is also a need for pragmatic trials that compare tezepelumab head-to-head with other biologics in real-world settings. Such studies could help clarify which patients benefit most from each agent and inform treatment algorithms. The UK's National Institute for Health Research (NIHR) has funded a feasibility study for a randomised registry trial, but results are not expected for several years.
The real-world data from the UK provide a strong signal that tezepelumab can halve asthma attack rates in a broad population of patients with severe disease. But the drug is not a cure, and its place in the treatment algorithm will continue to evolve as more evidence accumulates. For now, it offers a valuable option for patients who have run out of others — and a reminder that understanding the upstream biology of inflammation can lead to therapies that work where others fail.
This article is for informational purposes only and does not constitute medical advice. Patients should consult their healthcare provider about treatment options.